One group that I seemed to have not written about yet is mothers. So I would like to dedicate this post to the discussion of postpartum depression and race. In my opinion, in at least understanding the intersection between postpartum depression and race, a dialogue surrounding the socio-cultural and environmental factors of postpartum depression. This is in turn can lead to a dialogue how to support these mothers and potentially how to strategically minimize this type of depression.
After doing a quick search online, I came across this article.
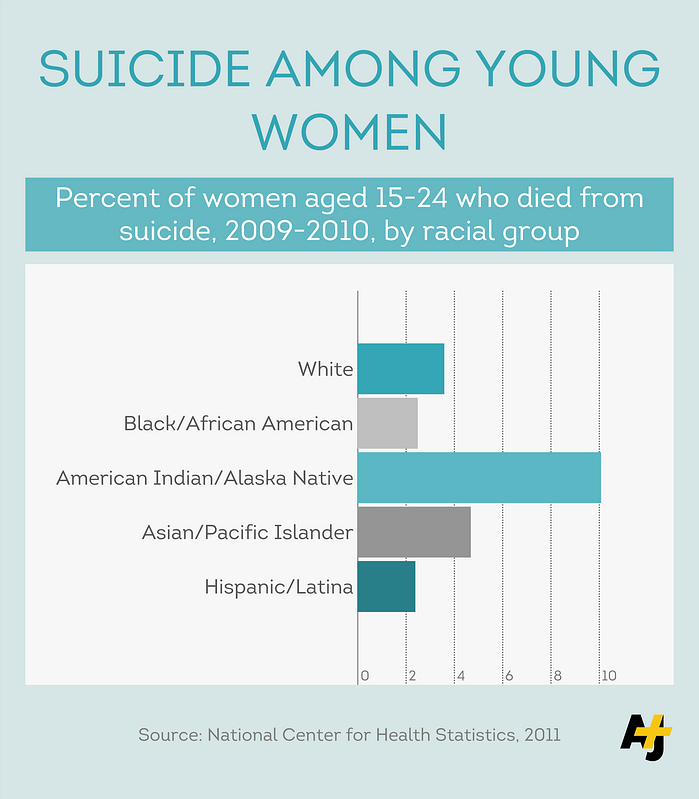
The key idea to pull this from this article is: “Statistically, postpartum depression can be ranked from high to low as Native Americans, Whites, African Americans and Hispanics”.
So the question is why? Why is it that Native American women have the highest levels of postpartum depression? (Of course there are other factors and identities that inform this but it is still a valid question to pose).
The first idea come to my mind is the disproportionate violence that indigenous women face. Trauma and violence experienced throughout a lifetime can certainly inform ‘potential’ to depression.
On the flip side, why is that Hispanic women experience the lowest levels? What factors within the Latina community may provide for better support systems during pregnancy?
As a final thought, how accurate is this study at all? What other identities were considered throughout this study, if any?
{kind=link}